REST vs WebSocket for Vitals Streaming: Which to Choose in 2026
REST vs WebSocket for vitals streaming API integration — a practical comparison of latency, throughput, and architecture trade-offs for health platform developers in 2026.
REST vs WebSocket for vitals streaming: which to choose in 2026
If you're building a health platform that captures vital signs from a camera-based SDK, you'll hit this decision pretty early: do you stream vitals data over REST or WebSocket? The REST vs WebSocket vitals streaming API choice isn't academic. It changes how your app feels to end users, how your backend scales, and how much you'll spend on infrastructure when the user base grows.
The short answer is that both work, and most production systems end up using both for different parts of the pipeline. But the details matter more than the architecture diagram.
"WebSocket maintains an open connection, meaning there is no need to establish a new connection with each data update. This significantly reduces latency compared to REST API, where each request involves establishing a new connection." — Arif Rahman, Python in Plain English, 2025
How REST and WebSocket actually differ for vitals data
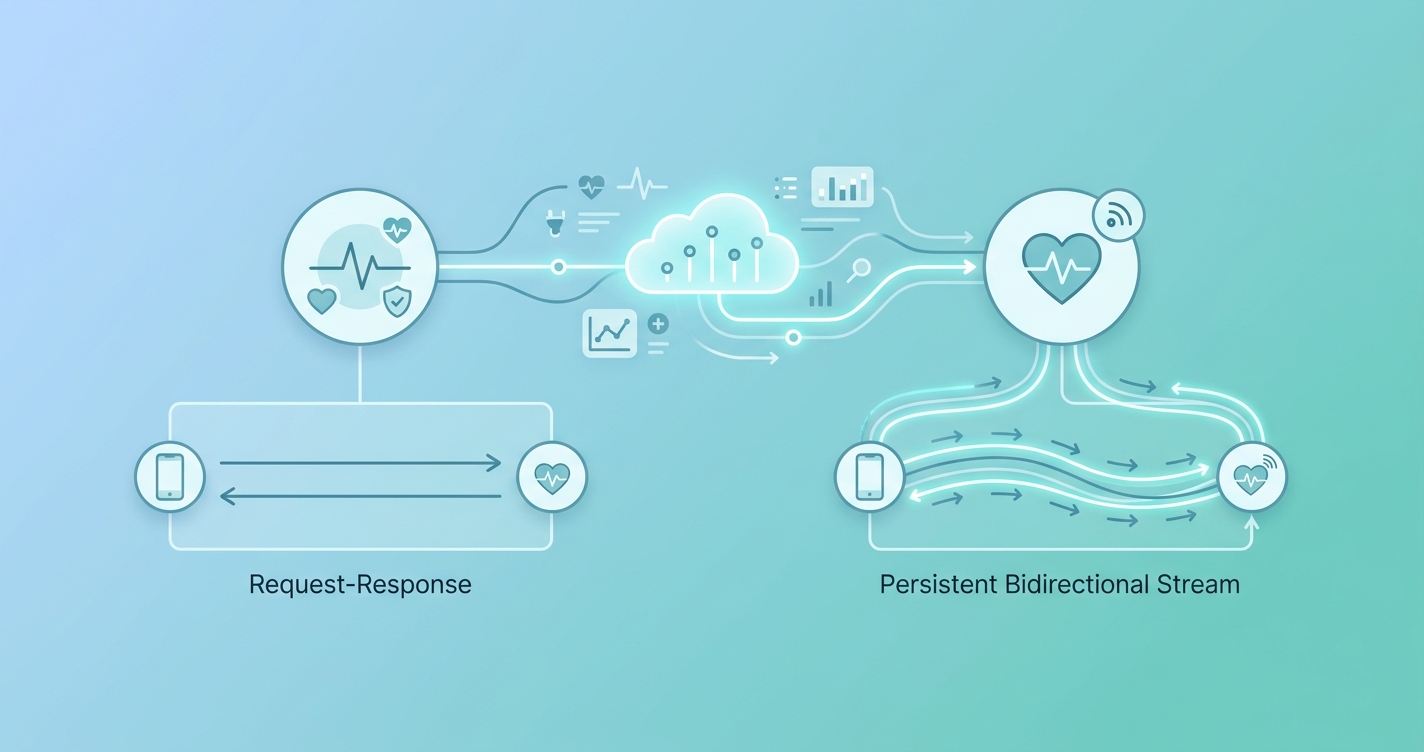
REST is request-response. Your client asks for something, the server sends it back, the connection closes. For vitals, that means either the client polls at some interval ("give me the latest reading every 2 seconds") or the server batches readings and the client fetches them periodically.
WebSocket is a persistent, full-duplex connection. Once the handshake completes, both sides can send data at any time without the overhead of new HTTP headers, TCP handshakes, or TLS negotiations on every message. For a vitals SDK that produces readings at 30Hz during a face scan, that difference compounds fast.
The overhead gap is real. Each REST request carries HTTP headers that typically add 200-800 bytes per call. A WebSocket frame carrying the same vitals payload adds about 2-6 bytes of framing overhead. When you're sending heart rate, SpO2, and respiratory rate readings multiple times per second, those extra bytes become meaningful at scale.
Research published by the Scientific Research Publishing group found that WebSocket connections consumed roughly 50% less bandwidth than equivalent HTTP polling for the same data throughput, with round-trip latency dropping from hundreds of milliseconds to single-digit milliseconds on local networks.
| Factor | REST API | WebSocket |
|---|---|---|
| Connection model | New connection per request | Persistent, reused connection |
| Latency per message | 50-200ms (includes TCP/TLS setup) | 1-10ms (frame only) |
| Header overhead per message | 200-800 bytes | 2-6 bytes |
| Direction | Client-initiated only | Bidirectional |
| Bandwidth at 10 msgs/sec | ~8-10 KB/sec overhead | ~0.06 KB/sec overhead |
| Caching | Native HTTP caching | No built-in caching |
| Load balancer support | Standard | Requires sticky sessions or L7 support |
| Reconnection handling | Automatic (stateless) | Must implement reconnection logic |
| Browser support | Universal | Universal (since 2011) |
| Firewall compatibility | Passes everywhere | Occasionally blocked by corporate proxies |
When REST is the right call for vitals
Not every vitals integration needs real-time streaming. Some of them are better off with REST, and overengineering the transport layer is a real thing.
On-demand readings
If your application captures vitals once (a 30-second scan, for example) and then displays results, REST is simpler and works fine. The user scans, the SDK processes locally, the client POSTs the result to your server. One request, one response. Done. There's no persistent connection to manage, no reconnection logic to write, no WebSocket library to bundle.
Batch uploads and historical data
When a mobile app collects vitals periodically throughout the day and uploads them in batches — say, four readings taken during morning, midday, afternoon, and evening check-ins — REST handles this cleanly. You're sending a JSON array of timestamped readings in a single POST. The request-response model maps perfectly to batch operations.
EHR integration layers
Most Electronic Health Record systems expose FHIR-compliant REST APIs. HL7 FHIR, the dominant interoperability standard for healthcare data exchange, is built on REST conventions. If your vitals data needs to land in an EHR, you're almost certainly going through a REST endpoint regardless of how the data got to your server. The Office of the National Coordinator for Health IT (ONC) has pushed FHIR adoption aggressively since the 21st Century Cures Act, and by 2026 nearly every major EHR vendor supports FHIR R4 endpoints.
A practical architecture: stream vitals over WebSocket between the SDK and your application server, then relay processed readings to EHR systems over REST/FHIR. Each protocol handles what it's good at.
When WebSocket wins for vitals streaming
Live monitoring dashboards
If a clinician watches a patient's vitals in real time during a telehealth visit, WebSocket is the clear choice. Polling a REST endpoint every second creates unnecessary load and still introduces up to a full second of display lag. WebSocket pushes each reading the moment it's processed.
A 2025 analysis in the International Journal of Engineering Trends and Technology measured WebSocket round-trip times at 48-52 milliseconds over cloud connections, compared to HTTP polling at 180-240 milliseconds for equivalent payloads. For a dashboard showing heart rate that updates with every beat, that gap is the difference between feeling live and feeling laggy.
Multi-vital concurrent streams
Camera-based rPPG SDKs don't produce a single number. During a scan, they might output heart rate, heart rate variability, respiratory rate, blood oxygen estimation, and stress indicators — all at slightly different intervals. Multiplexing these streams over a single WebSocket connection is straightforward. Doing the same over REST means either bundling everything into one polling endpoint (which means you're limited by the slowest vital's update rate) or running parallel polling loops (which is wasteful).
Alerting and threshold notifications
When vitals cross a clinical threshold, you want the server to push an alert immediately. REST can't do this without long-polling or server-sent events, both of which are workarounds for the fact that REST isn't designed for server-initiated communication. WebSocket handles this natively — the server sends an alert frame the moment a reading triggers a threshold, with no client polling delay.
Architecture patterns that work in production
Most health platforms that reach production scale don't choose one protocol exclusively. They use both, matched to different parts of the data flow.
The common hybrid pattern
[SDK on device] → WebSocket → [App Server] → REST/FHIR → [EHR/Data Store]
↓
WebSocket → [Live Dashboard]
↓
REST → [Analytics/Batch Processing]
The SDK streams raw vitals data over WebSocket to the application server. The server processes, validates, and stores readings. Live dashboards subscribe over WebSocket for real-time updates. Historical queries, batch exports, and EHR integrations use REST.
Connection management matters more than you think
WebSocket connections are stateful, which makes horizontal scaling harder than REST. If your app server runs behind a load balancer, you need either sticky sessions (so a client's WebSocket always hits the same server) or a pub/sub layer like Redis that broadcasts vitals across server instances.
Censinet's 2025 analysis of IoT monitoring protocols in healthcare environments noted that "HTTP/REST remains a popular option due to its simplicity and compatibility with web services and clinical applications. However, its stateless design and header overhead can result in latency and bandwidth inefficiencies for continuous monitoring." Their recommendation: use WebSocket or MQTT for the real-time leg, REST for everything else.
| Architecture pattern | Best for | Complexity |
|---|---|---|
| REST only | Single-scan apps, batch uploads | Low |
| WebSocket only | Live monitoring, real-time alerts | Medium |
| Hybrid (WS + REST) | Full-featured health platforms | Medium-high |
| MQTT + REST | IoT devices with constrained bandwidth | High |
| SSE + REST | One-way server push, simple dashboards | Low-medium |
Security considerations that are specific to vitals
Vitals data is protected health information under HIPAA (in the US) and equivalent regulations elsewhere. The transport choice affects your compliance posture.
REST over HTTPS encrypts each request independently. WebSocket over WSS (WebSocket Secure) encrypts the persistent connection. Both use TLS, so the wire-level security is equivalent. The difference is in access control patterns.
REST APIs typically authenticate each request with a bearer token. If a token is compromised, the blast radius is limited to whatever that token can access. WebSocket connections authenticate once at the handshake and then stay open. A compromised WebSocket connection gives continuous access until the connection is terminated or the token expires.
For vitals streaming, implement token refresh within the WebSocket connection. Send a re-authentication frame before the token's expiry, and have the server drop connections where the token has lapsed. Most WebSocket libraries don't handle this out of the box, so plan for it.
Current research and evidence
The academic literature on real-time health data transport has grown substantially. A team at the University of Oulu published work in 2024 comparing WebSocket and REST performance for wearable health monitoring systems, finding that WebSocket reduced battery consumption on mobile devices by 15-23% compared to equivalent REST polling, primarily because the radio stayed active for shorter periods with push-based delivery versus periodic polling wake-ups.
CapMinds, a healthcare IT consultancy, published a detailed analysis of FHIR Subscription APIs in 2025, documenting the shift from batch processing to real-time event-driven pipelines in clinical monitoring. Their finding: "Traditional healthcare systems rely heavily on batch processing and periodic data updates, which are frequently too slow for critical clinical situations." FHIR R5 introduces a Subscription resource that supports WebSocket as a channel type, bridging the gap between real-time streaming and healthcare interoperability standards.
The Internet Engineering Task Force (IETF) RFC 6455 defines the WebSocket protocol, and its adoption in healthcare has been steady since browser support became universal. MQTT, another persistent-connection protocol originally designed for IoT, has also gained traction in medical device streaming — the International Journal of Engineering Trends and Technology published latency benchmarks in 2025 showing MQTT and WebSocket performing comparably at 48-94ms round-trip over cloud infrastructure, both substantially outperforming HTTP polling.
The future of vitals streaming APIs
FHIR's evolving support for real-time channels will likely reshape how vitals flow between systems. The FHIR R5 Subscription framework allows servers to push updates over WebSocket, which means the artificial boundary between "real-time transport" and "interoperable health data exchange" is collapsing. Developers who build WebSocket streaming now will have a smoother migration path as FHIR R5 adoption grows.
HTTP/3 and QUIC may also change the calculus. QUIC reduces connection establishment time significantly compared to TCP+TLS, which narrows the latency gap between REST-style requests and persistent connections. It won't eliminate the per-request overhead problem, but it makes REST less painful for moderate-frequency vitals polling.
For SDK providers like Circadify, the trajectory is clear: offer both transport options, with WebSocket as the default for real-time use cases and REST for integration with existing healthcare infrastructure. The SDK handles the hard part — extracting vitals from camera data — while the transport layer adapts to whatever the platform needs.
Frequently asked questions
Can I use REST polling instead of WebSocket for live vitals display?
Technically, yes. Practically, polling at sub-second intervals creates significant server load and still introduces latency. If your dashboard needs to feel responsive — updating with each heartbeat, for instance — WebSocket is worth the added complexity. For updates every 5-10 seconds, REST polling is fine.
Does WebSocket work through corporate firewalls?
Most corporate firewalls pass WebSocket traffic because it upgrades from a standard HTTPS connection. Some aggressive proxy servers that perform deep packet inspection may interfere, though. If your health platform serves enterprise clients, test WebSocket connectivity from behind their network infrastructure before committing to it as the only transport. Having a REST fallback is good practice.
How do I handle WebSocket disconnections during a vitals scan?
Implement automatic reconnection with exponential backoff. Buffer vitals readings on the client side during the disconnection window and replay them once the connection reestablishes. Most production WebSocket libraries (Socket.IO, SignalR, native browser WebSocket with a wrapper) support this pattern. The buffering is the part you need to build — don't lose readings just because a connection blipped for 2 seconds.
Is MQTT better than WebSocket for health device streaming?
MQTT was designed for constrained IoT devices and works well in that context — low bandwidth, unreliable networks, tiny payloads. For browser-based or mobile SDK integrations where the client is a smartphone or web app, WebSocket is more natural because it's a web-native protocol. MQTT adds a broker layer that may be unnecessary if your vitals flow directly from app to server. That said, if you're building for medical IoT devices or clinical kiosks with limited resources, MQTT deserves evaluation.